Sharing knowledge and experience on quality improvement for community health and sustaining change
USAID SQALE Learning Event Report 2019
USAID SQALE has regularly held learning events to help stakeholders in the Kenyan community health system communicate the results of their quality improvement interventions, share lessons learned and strategise about next steps. This multi-media report outlines what changes have happened in community health, the impacts that USAID SQALE has had on national level policy and tools, and how communities and health care staff plan to sustain positive change in the longer term. Here is a list of participants...
The USAID SQALE learning event was the third and most ambitious learning event supported by the USAID SQALE Programme over the last three years. It was a chance to share and learn across Nairobi, Migori and Kitui counties, to celebrate success in implementing community led quality improvement (QI) and recognise innovative high performing Work Improvement Teams. At the learning event we also heard more about the research findings from USAID SQALE and planned for how to sustain the gains that we have made after the project funding finishes. Finally, we were delighted to use this event as a chance to launch the national KQMH Facilitators Manual for Quality Improvement in Community Health Services, which we developed in collaboration with the Ministry of Health.
Dr Nganga, from Nairobi County Ministry of Health welcomed the USAID SQALE teams to Nairobi and stressed the importance of learning and sharing with one another.
Sustaining Change, making an impact. Long live the Quality Revolution!
A rousing keynote address from Vicki Doyle got participants motivated and excited for the days ahead. Read the full speech...
Quality Improvement: Making a difference at county level
Representatives from Kitui, Migori and Nairobi counties provided an overview on how the USAID SQALE program has made a difference.
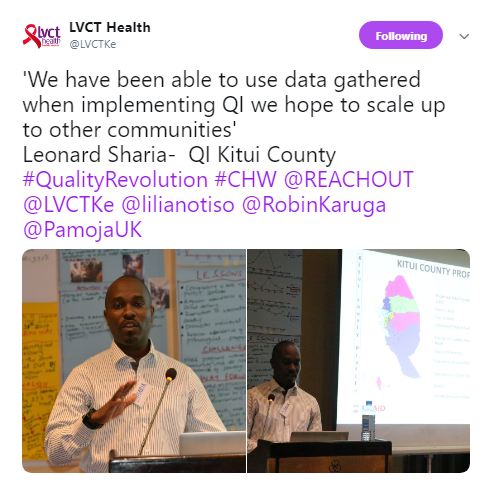
Kitui county is large with over 1.1 million people, it is a challenge to cover all the population. We have eight sub-counties and we are implementing QI in three of them Kitui East, Mwingi North and Kitui Central. We have 247 Community Health Units (CHUs) with eight to ten Community Health Volunteers (CHVs) per unit. Research from LVCT Health demonstrated a number of challenges in the community health program which led to change, for example, paying CHVs a stipend and changing CHV distribution, training, engagement and supervision. We have set a budget so we can continue to pay CHVs and we funded coaching in two sub-counties. We chose the theme of skilled deliveries for QI and we were able to increase the number. Implementing QI at the community level is key to the provision of efficient community services, it improves data quality and use and therefore decision making. Implementing QI at the community level does not need large amounts of resources as it entails simple approaches.”
Leonard Sharia (Kitui County)
“We have 177 CHUs and 2130 CHVs who are paid a stipend. We have implemented QI in Nyatike, Suna West and Kuria West. We are developing a Community Health Services Bill and this is important because we want to ensure that the stipend is enshrined in law so that regardless of who takes over the CHVs will be paid. We have conducted an LQAS survey on equity. The county WIT Technical Working Group brought together all partners involved in Community Health Services and set QI indicators to enhance quality across the county. We held a Community Health Summit which was a splendid learning opportunity and Afya Halisi have scaled this up in other sub-counties. Teamwork is important for QI implementation - from the county all the way to the community. Community QI can be scaled up to other communities and facilities. It made CHUs appreciate the value of data. In the communities we focused on there was a magnificent change in the indicator that we chose.”
Tom Odhong’ (Migori County)
“60% of Nairobi’s population lives in informal settlements. Each CHU has 1000 households and the CHVs have no stipend. If the Community Health Services Bill is passed, then we will start paying them. We have cascaded QI in all our sub-counties scaling up from the three that LVCT Health is active in. We have been doing quarterly supportive supervision and Data Quality Assessments (DQAs). We have concentrated on completion of four antenatal care (ANC) visits. We learned that the process of QI strengthens the community-facility linkage and community services more generally. Recognition of good practice is a motivator. The Community Follow Up Tool allowed us to hear the voice of the community. We are leveraging on enrolment of households into the National Health Insurance Fund. We will now scale up in other CHUs and take up a new theme.”
Judy Macharia (Nairobi County)

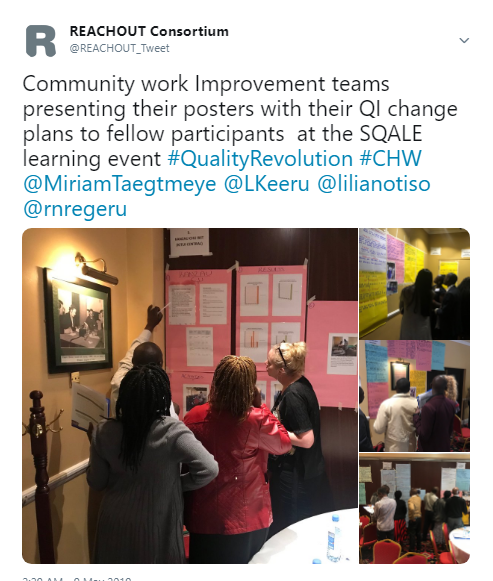
Poster presentations
The poster presentation session was one of the longest but most informative sessions of the USAID SQALE learning event. The walls of the meeting room were covered with a collage of rainbow coloured charts that represented three years of work.
Poster presentation teams were made up of members of the WITs and included Community Health Extension Workers (CHEWs), Facility-in-Charges, CHVs and community members.
As participants rotated round the room to hear lightening presentations from each speaker the noise in the room rose to a crescendo. Every ten minutes the hubbub would be broken by an ear-splitting whistle as our moderator Mike prompted us to move on to the next presentation and order was briefly restored.
There was a palpable tension in the room as presenters gave it their all, vying to win the coveted Learning Event Awards. Occasionally the voices of the moderators would be heard as they called on to the different presenters to wind up.
The posters were developed with the guidance of LVCT Health technical officers according to a template during QI coaching in WIT meetings. They covered the following headings:
- Problem identification, prioritization and development of problem statement
- Root cause analysis
- Development of solutions to formulate QI Change Plans
- Implementation and testing if changes make a meaningful impact
Teams also documented their work in the community with photography which were scrutinised by the judges that roamed the rooms.
As the session drew to a close tired participants and judges - who had either judged or presented nine times during the sessions – took their seats and reflected on the huge amount of work and inspiring stories of improvement that had been summarised in the session.
World Café on Key Issues for the USAID SQALE Program
The world café method is used in large meetings to create an interactive environment for knowledge sharing. It allows everyone to contribute, connecting different perspectives and allowing moderators to look for patterns and insights. Several tables were set up with a moderator and a note taker who were focused on a particular topic:
- Sustaining QI
- Collaborating for Quality Improvement of community health services
- Quality Improvement Impact
- Innovating for community engagement
- Helping communities to be more resilient
- Communicating data
- Informing the Community Health Strategy
The session began hesitantly as participants were introduced to the topics under discussion. But after a few minutes they gained confidence and naturally started airing their views and chatting.
Sustaining QI
USAID SQALE funding is coming to an end. We asked participants how they would sustain the momentum of their work on QI once the project stops. Read more...
Collaborating
Quality improvement encourages a multi-disciplinary team approach to problem solving, monitoring and ultimately improving the quality of community health services. This session enabled participants to feedback on what is working well and what should change. Read more…
Making an impact
One of the core principles of QI in Community Health Services is the use of data to analyse working practices and whether we are meeting minimum standards for service delivery. This session focused on how WITs measure impact and what monitoring and evaluation activities are in place. Read more…
Community engagement
If we want to improve the quality of community health services and achieve Universal Health Coverage we need to engage with hard to reach populations. During the USAID SQALE implementation period, there have been different levels of interaction with the community. This session explored the different types and levels of engagement within the community. Read more…
Community resilience
Community resilience is the sustained ability of communities to withstand, adapt to, and recover from disasters, shocks, unexpected events etc. In many ways, health is a key foundation of resilience because almost everything we do to prepare for disaster and protect infrastructure is ultimately in the interest of preserving human health and welfare. Participants discussed how the QI skills that they had developed during USAID SQALE could be applied in other areas. Read more…
Using data to communicate
Improving data quality and enhancing potential users’ ability to collect analyse and apply data has been central to the USAID SQALE approach to quality improvement. In this session participants fed back on what formats and mechanisms have been most useful and what more could be done. Read more…
Informing the Community Health Strategy
QI work at the county and national level has led to the voices of community members and health workers being heard in discussions about policy and standards. This session allowed participants to explore what more could be done to feed into national policy and some of the key messages that people wanted pushed forward. Read more…





“We need to send the stories of QI to the politicians so that you become a learning site for others to take your expertise from. Although USAID SQALE is scaling down, the ideas and the structures that have been created can endure. It can also be scaled up to other counties. I would like to thank all the foot soldiers for QI at the community level for their efforts.” Dr Charles Kandie, Head, Department of Health Standards and Quality Assurance
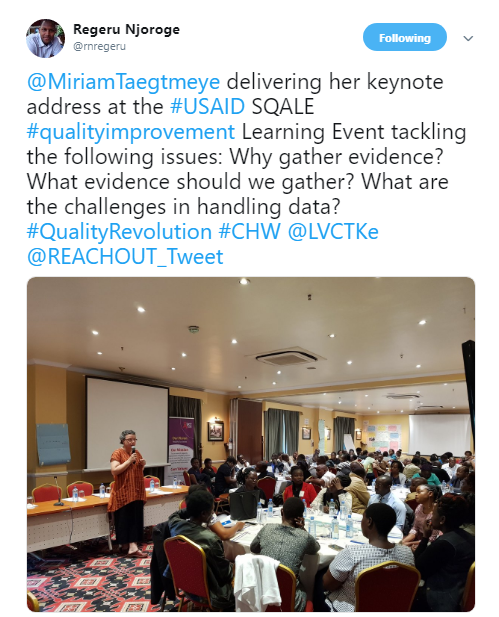
Gathering evidence for equity in community health
A keynote address from Professor Miriam Taegtmeyer explored ideas around evidence and the importance of learning from community knowledge. Read the full speech…
“USAID are delighted to have partnered with LSTM and all of you have demonstrated that community QI can be institutionalized. We want to prevent our mothers and children from dying. I am excited that in Nairobi and Migori, we have a budget for CHVs’ stipends. My call to you is that in the counties we are working, we need to strengthen our collaboration with other partners working there. What we have done over the past three years should not die, it should continue and we should be champions of QI.” Sila Kimanzi, Project Management Specialist (Child Health/WASH), USAID
Panel discussion
In a panel discussion, which was moderated by Dr Lilian Otiso, representatives from Nairobi, Migori and Kitui counties reflected on the process of implementing the USAID SQALE program and its impact. The panellists included Judy Macharia (CHS Focal Person, Nairobi County, Tom Odhong’ (CHS Focal person, Migori County), Mike Okinyi, Mary Njonde (Facility-in-charge, Nairobi), Thomas Muniko , Gladys Mutinda (Ifya Uzazi) and Malcom Odhiambo (CHS Focal Person, Kitui Central).
Data for decision making
In Migori they have started DQA and mapping and tracking of pregnant mothers to ensure that they are visited by a CHV each month and that they complete at least four ANC appointments. In Kitui DQA auditing has helped bring out issues in the community that are addressed by WITs and articulated to the CHVs. This has translated into improvements in data collection.
The view from the county level
Tom explained how the County Health Management Team has institutionalised the use of community QI feedback by including it as an agenda item in their regular Monday morning briefs. Through collaboration with other partners they have trained around 445 health care providers on QI. They have replicated the style of the learning events at the facility, where people make presentations, and this has helped them own their data. He reported that they have scaled up in four CHUs outside the USAID SQALE supported sites which was made possible through the support of Afya Halisi. CHEWs and public health officers have had their capacity built. In the Annual Work Plan 2019-2020, community health has received a budget of about 8 million Kenyan Shillings, with a focus on community QI. The perennial challenge is the fact that funding is very erratic at county level.
To Judy from Nairobi community QI was God sent. Their reporting rates and timeliness used to be at 30%-40% but now they are nearer 95%. Afya Halisi helped them to train the nurses and CHAs on data quality audits and this has spread in new sub-counties. Improved data quality has been prompted by improved reporting rates and completeness and timeliness of data. She explained that before USAID SQALE they had less than 10% coverage and now they are at 53%. Their data assisted us with advocacy and led to interest from other development partners and AMREF and PharmAccess are supporting them as a result. Community QI helped them to tell the national level that they needed to look at and revise their reporting tools because they were not capturing the information that was required. The CHVs are now enrolling houses into the NHIF. They have been provided with energy and support through the improvements in supportive supervision prompted by REACHOUT. CHVs are also motivated through the exercise of rewarding and recognizing the best performing CHUs, during learning events. In terms of budget they are finalising the budget for 2019-2020 and community QI has been budgeted for 7.8 million Kenyan Shillings which includes coaching, DQA and supportive supervision. CHVs in Nairobi will be getting a stipend from July 2019.
Taking forward QI in the community
Gladys felt that as a result of the USAID SQALE program CHV consciousness of quality has improved. Furthermore, CHVs have a better understanding of the importance of the work that they do. They know that the evidence that they collect is used for learning and decision making. At community level they have champions that do the coaching in the facility and they will stay and sustain QI over the longer term.
Njonde believed that learning from the community could be useful at facility level. For example, the USAID SQALE Community Follow Up Tool could be adapted to enable the facility to follow up on their work. They would also like to have a tool that allows them to have an exit interview to gauge how services are being offered at the facility and what the clients feel about the services they are receiving.
Michael argued that WIT meetings and composition should be extended. Community Health Committees should be integrated into the WITs to bring more ideas on board and reach more people. Their main way forward is to cascade community QI to other WITs and hope to receive budget support from county.
The links between community QI and Universal Health Coverage
Tom felt that to achieve UHC there needs to be consistent supportive supervision focused on Community Health Services. Consistent coaching and mentorship for health care providers is also important. To sustain action in this area they will hold a CHS summit every December and other learning and sharing events will be organized at county and sub-county levels. Coaches trained by USAID SQALE will mentor other health care providers in the county.
Judy argued that without QI, embedded in both communities and facilities, there is no UHC. So QI needs to be included in annual workplans and embedded in service delivery. They will continue to use the Community Follow Up Tool which helps managers to understand whether community members accept the services that they are receiving from CHVs. She pointed out that they have raised the voice of the community in discussions about the revision of CHS indicators and the monitoring and evaluation framework for CHS is being altered in the light of these inputs.
Malcolm pointed out that some of the CHVs are having to photocopy their own tools to report on a monthly basis. There are almost 100 chalkboards that can’t be used as they are for negative indicators. There is a need to constantly revise tools and make them available. He recommended that this needs to be a part of the new CHS policy at national level.




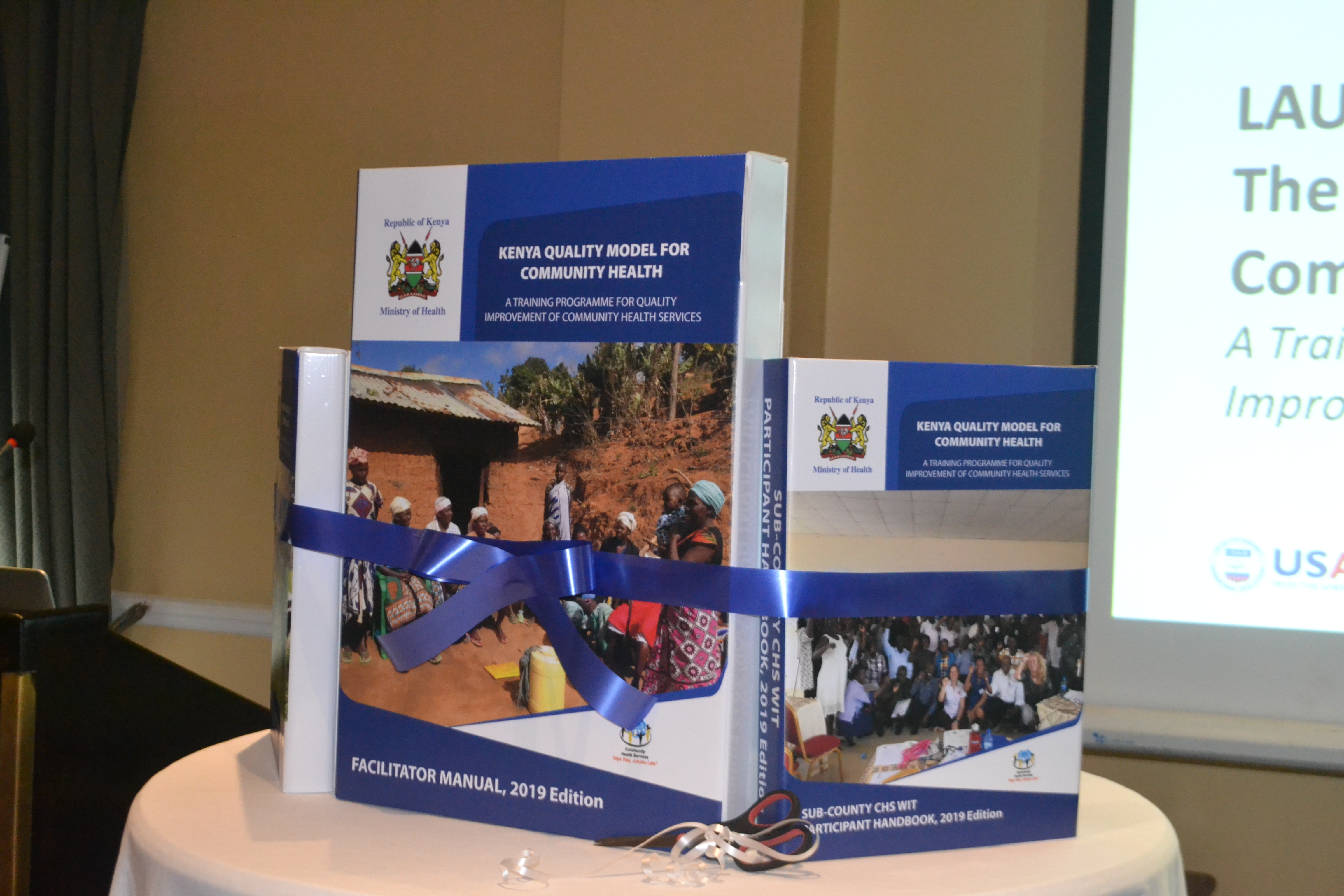
Launch of the KQMH Facilitators Manual
Based on learning and evidence from the USAID SQALE programme, a facilitators’ manual and participants handbook has been piloted and fully updated to reflect the practical reality of QI within Kenya’s community health system. The learning from this process has been embraced by the Ministry of Health and in this session we launched these new publications.
The KQMCH Facilitators Manual has been developed to train sub-county and community WITs in QI for community health services. The manual and participant handbooks are directed at managers, supervisors and coaches involved in community health, working at county and sub-county levels; and health care providers and community health volunteers working at community level
To ensure training is useful, simple and likely to be taken up at county level the manual was developed with the following guiding principles:
- Aligned with Kenya Quality Model for Health standards, national policy and country priorities.
- Reflects the latest thinking in QI, sourced from published literature and QI experts.
- Built on international and local research.
- Iterative user-centred design process involving stakeholders from community, sub-county and national level.
- Supports knowledge exchange between community and sub country levels.
- Empowers community health workers to take ownership of the QI programme and become QI champions.
- Structured to allow for additional content/ modules.
The KQMCH training and capacity building approach aims to improve health outcomes by embedding quality into the scale-up of community health services in Kenya. This is through a process of capacity building and community engagement that is delivered through the development and coaching of WITs for CHS at sub-county and community levels.

USAID SQALE research findings
Research has been a key component of the USAID SQALE program. In this session participants were able to hear a summary of findings from researchers working on the project and had time to interrogate the analysis, ask questions and provide their own interpretations of the data. The topics covered included the LQAS survey on equity, costing community QI, community participation mechanisms and posters and presentations that have been made by the research team at the Health Systems Global Conference.
LQAS
LQAS is a household survey method that is commonly used for baseline and follow-up assessments to assess the coverage of services provided especially where resources are limited. We studied the coverage of MNCH services at community level in three sub-counties (Nyatike, Kuria West and Suna West) in Migori County. We compared this with three non-USAID SQALE sub-counties (Suna East, Kuria East and Uriri). Read more about our findings…
Cost of QI at community level
To support the sustainability of the USAID SQALE program we conducted research on the cost of implementing QI in the community and have supported teams to find alternative routes for fundraising at the county-level and through development donors. Read more about the findings…
Community participation
Community Health Committees (CHCs) have been shown to deepen community engagement and responsibility in health decision-making. This research sought to improve our understanding of how and what contextual factors influence CHCs. It is hoped that the findings will help unlock the potential of CHCs to engage with communities and provide leadership in the improvement of community health services. Read more about the findings…
Health Systems Global
The USAID SQALE attended and presented at the Global Symposium on Health Systems Research in 2018. They facilitated a panel as well as giving poster presentations. This session provided a chance for community, county and national stakeholders to see how their work has been represented at the global level. Read more about the findings…
"No more blame game. We own the community health data now." Tom Odhong’, CHS Focal person, Migori County
Talking Wall: Consolidation of learning and sustainability planning
The talking wall session enabled participants to visually capture key lessons from USAID SQALE learning, to develop WIT and stakeholder sustainability plans post USAID SQALE funding and to publicly declare their commitment to continuing the Quality Revolution. The trees contain roots, which represent the foundations of learning generated by implementing the program. The fruits on the branches are the impacts that we have seen as a result of community QI.
Each team brainstormed the priority actions that would be required to sustain QI efforts and make an impact in their communities. These were displayed as a public commitment to the next steps they will take. WITs were very positive about sustaining change over the longer term.
Among county and sub-county WITS some of the most common plans were to: support the capacity building of CHVs in community QI and add more CHUs; to conduct quarterly DQAs; continue with supportive supervision; ensure that the appropriate tools are available; hold regular Learning Events; input into CHU Bills. Many pledged to incorporate these activities into annual workplans and to fundraise for them. Community WITS focused on: expanding income generating activities; monthly meetings and regular supervision; mapping pregnant women in their communities and the creation of mother-to-mother support groups; starting youth clubs; community dialogue and action days; engaging opinion leaders to advocate for QI; administering the Community Follow-Up Tool and offering capacity building support to other CHUs who have not yet started with QI.


QI Awards
We ended the learning events with the QI awards. The QI awards are a chance to celebrate excellence in community health services. This time the competition included the categories of best poster, best photo and caption, QI impact at sub-county level, QI impact at CHU level, increased household visits per CHU and increased household visits per sub-county. Here is a list of all the winners!